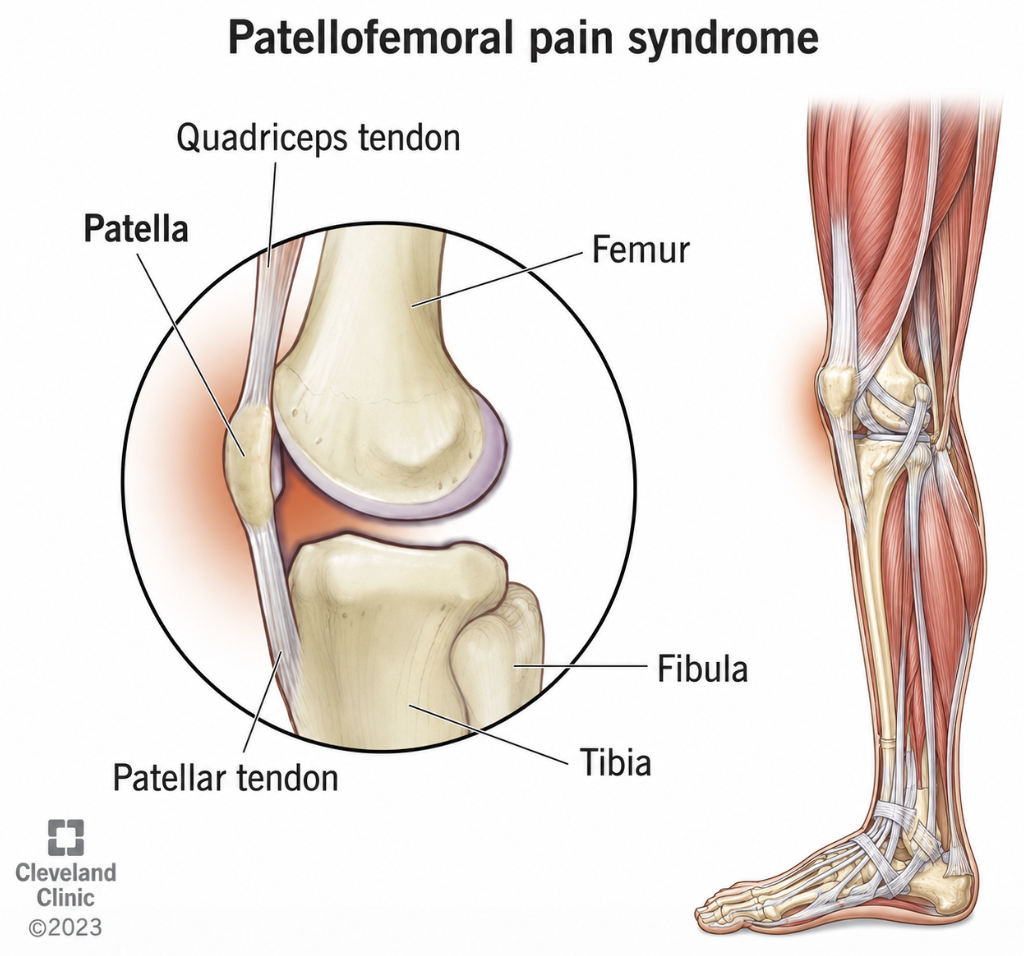
Do your knees ache when you go downstairs, squat, run, or sit for too long? If so, you may be dealing with patella femoral pain syndrome—often called “runner’s knee.” Although the name sounds complicated, the idea is simple: the area around or behind your kneecap becomes irritated when the knee is loaded, especially during bending activities.
A recent randomized controlled trial found that combining electrical stimulation with hip and knee strengthening helped people with patellofemoral pain improve pain, function, knee strength, and movement during stair descent compared with strengthening alone (Yang et al., 2026). In other words, a smart rehab plan may help your knee feel better and move better. If this is something that you struggle with Book an Appointment today.
What Is Patella Femoral Pain Syndrome?
Patella femoral pain syndrome, also called patellofemoral pain or “runner’s knee,” is pain around or behind the kneecap. Usually, it gets worse when the knee is bent under load. For example, you may notice pain with stairs, squats, lunges, running, jumping, kneeling, or sitting with your knees bent.
Essentially, the kneecap and thigh bone need to work together smoothly. However, if your hip, thigh, foot, or knee control is off, the kneecap may become irritated. As a result, everyday movements can start to feel painful.
Who Is Most at Risk?
Although anyone can develop patellofemoral pain, it is especially common in active people. You may be at higher risk if you:
- Run, jump, squat, or climb stairs often
- Recently increased your workouts too quickly
- Have weak hip or thigh muscles
- Have poor knee control, such as the knee dropping inward
- Play sports with cutting, landing, or repeated jumping
- Spend lots of time sitting, then suddenly return to activity
Additionally, students, runners, gym-goers, and weekend athletes may notice symptoms when training volume changes with the season.
What Does It Take to Get Better?
First, recovery usually takes consistency. While rest may calm symptoms temporarily, it often does not fix the reason the knee became irritated. Instead, most people need a progressive plan that gradually builds tolerance.
Typically, rehab includes:
- Reducing painful overload at first
- Strengthening the hips, quads, and calves
- Improving squat, stair, running, or landing mechanics
- Gradually returning to sport or gym activity
- Using taping, education, or temporary activity changes when helpful
Importantly, research supports exercise therapy, especially a combination of hip-focused and knee-focused exercises, to reduce pain and improve function (Collins et al., 2018).
How Can Physiotherapy Help?
Physiotherapy can help by identifying what is actually driving your symptoms. For instance, your physiotherapist may assess your strength, walking, stairs, squat form, hip control, flexibility, and training routine.
Then, your plan may include targeted stength training and strength training exercises, movement retraining, hands-on care when appropriate, and education on how to return to activity safely.
In the Yang et al. study, both groups completed hip and knee strengthening for 6 weeks. However, the group that also received electrical stimulation to the vastus medialis—the inner quad muscle—showed greater improvements in knee extensor strength, muscle activation balance, pain, function, and movement patterns during stair descent (Yang et al., 2026). Therefore, electrical stimulation may be a useful add-on in some cases, especially when quad activation is a problem.
Do not attempt unless you have been assessed and cleared to attempt these by a licensed professional
People Also Ask
What is the best exercise for patellofemoral pain syndrome?
There is no single “best” exercise for everyone. However, the best starting point is usually a combination of hip and knee strengthening. Common options include step-downs, wall sits, bridges, side-lying hip raises, squats to a comfortable depth, and controlled leg extensions.
That said, the right exercise should feel challenging but manageable. If your pain spikes or lingers, the exercise may need to be modified. Best practice guide for patellofemoral pain based on synthesis of a systematic review, the patient voice and expert clinical reasoning.
What happens if patellofemoral pain syndrome is left untreated?
If left untreated, symptoms may become more persistent. As a result, you might avoid stairs, running, squats, or sports. Over time, this can lead to weakness, reduced confidence, and recurring flare-ups. Therefore, early treatment is helpful because it can address the cause before the problem becomes chronic. Factors that predict a poor outcome 5-8 years after the diagnosis of patellofemoral pain.
What triggers patellofemoral syndrome?
Patellofemoral syndrome is often triggered by too much load too soon. For example, suddenly increasing running distance, adding hills, doing deep squats, or returning to sport after a break can irritate the front of the knee.
Furthermore, poor hip and knee mechanics may add stress. If the hip rolls inward, the knee collapses inward, or the thigh muscles do not share the load well, the kneecap may experience extra pressure. Therefore, treatment should not only focus on pain—it should also address strength, control, and movement habits. Update of Risk Factors, Diagnosis, and Management of Patellofemoral Pain.
Helpful resources
For more reading, see the ChoosePT guide, and the AHS overview. For more help, visit Physiotherapy Services and Book an Appointment.
Ready to Get Back to Moving?
If knee pain is stopping you from training, working, or enjoying life, physiotherapy can help you take the next step. At our clinic in Edmonton, AB, we can assess your knee, build a personalized plan, and guide you through safe strengthening, movement retraining, and return to activity. Book an Appointment today with a physiotherapist and start moving with more confidence.
References
Collins, N. J., Barton, C. J., van Middelkoop, M., Callaghan, M. J., Rathleff, M. S., Vicenzino, B., Davis, I. S., Powers, C. M., Macri, E. M., Hart, H. F., de Oliveira Silva, D., & Crossley, K. M. (2018). 2018 consensus statement on exercise therapy and physical interventions to treat patellofemoral pain. British Journal of Sports Medicine, 52(18), 1170–1178.
Yang, X., Xue, B., Sun, D., Liang, M., Yao, Y., Yang, C., Zhou, Z., Gu, Y., Yu, P., & Xiang, L. (2026). Effects of electrical stimulation combined with strength training on pain, muscle strength and lower-limb biomechanics in patellofemoral pain patients: A randomized controlled trial. BMC Musculoskeletal Disorders, 27, Article 88. https://doi.org/10.1186/s12891-025-09465-3
Neal, B. S., Lack, S. D., Bartholomew, C., & Morrissey, D. (2024). Best practice guide for patellofemoral pain based on synthesis of a systematic review, the patient voice and expert clinical reasoning. British journal of sports medicine, 58(24), 1486–1495. https://doi.org/10.1136/bjsports-2024-108110
Lankhorst, N. E., van Middelkoop, M., Crossley, K. M., Bierma-Zeinstra, S. M., Oei, E. H., Vicenzino, B., & Collins, N. J. (2016). Factors that predict a poor outcome 5-8 years after the diagnosis of patellofemoral pain: a multicentre observational analysis. British journal of sports medicine, 50(14), 881–886. https://doi.org/10.1136/bjsports-2015-094664
Sisk, D., & Fredericson, M. (2019). Update of Risk Factors, Diagnosis, and Management of Patellofemoral Pain. Current reviews in musculoskeletal medicine, 12(4), 534–541. https://doi.org/10.1007/s12178-019-09593-z